
A post from the Stillbirth Advocacy Working Group stillbirths series by Sara Nam
More mothers are attending health facilities to deliver their babies, yet 2.6 million babies are stillborn every year, more than a third (42%) of those in Sub-Saharan Africa. What approaches can we apply to prevent stillbirths?
Pregnancy should be a time of joyful anticipation about the arrival of a new family member. But each year, 2.6 million babies are stillborn. Half these babies die during labour.¹
More than half a million of these are in Sub-Saharan Africa despite two thirds of all women giving birth in health facilities.¹
Most stillbirths are preventable through improved quality of care for pregnant mothers. Perinatal death review and response systems are an important mechanism to detect and address gaps in care. In developed nations, 10% of all stillbirths happen during labour compared to 51% in Sub-Saharan Africa.
Hannah Blencowe and Susannah Leisher’s blog point to the enormous social and economic returns if investments are made to the tracking and prevention of stillbirths.
What can be done to prevent stillbirths?
As a complement to tracking the number of stillbirths, we need to understand the cause of death and other circumstances during the mother’s pregnancy. Perinatal death reviews, or audits, are one way to do this. Evidence has found that as many as three out of every ten babies could be saved when the perinatal death review and response systems are implemented well.²
Perinatal death review committees investigate the care of the pregnant mother and the delays she may have faced in accessing care.
What are the challenges?
Committees often only review neonatal deaths and omit stillbirths. This is partly because there is more information in facility clinical records for a liveborn baby than one who is stillborn. All too often, there is not enough information to give a complete picture of what the factors were that contributed to a stillbirth.
Information is also missing when women have been referred form one facility to another or when women have come from a community far from the facility where the stillbirth took place.
What is needed?
We need to strengthen the information available for review committees so they can make informed decisions about how to improve the quality of care and prevent stillbirths.
We call upon implementers and clinicians to find ways to improve information that can be used for perinatal death reviews by:
a) Reviewing a selected sample of stillbirths as well as deaths of newborns
b) Ensuring each stillbirth or newborn death reviewed is done as comprehensively as possible
c) Improving the flow of communication between primary, secondary and referral facilities, including staff from all facilities involved in the care pathway in the perinatal death review where relevant
d) Involving communities or families in the perinatal death review process so they can provide information to guide recommendations and can implement recommendations at local level.
Too many babies die before they are born and during the intrapartum period when quality care should be able to prevent most stillbirths, and more information can help make perinatal death review and response systems improve quality of care.
REFERENCE
¹ Lawn, J., Blencowe H., Waiswa, P. et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. The Lancet Global Health. 2016;4(2): e98 – e108 2016.
² Pattinson R , Kerber K, Waiswa P, Day LT, Mussell F Asiruddin S, Blencowe H, Lawn JE. (2009) Perinatal mortality audit: Counting, accountability, and overcoming challenges in scaling up in low- and middle-income countries. International Journal of Gynaecology and Obstetrics 107 (2009) S113–S122
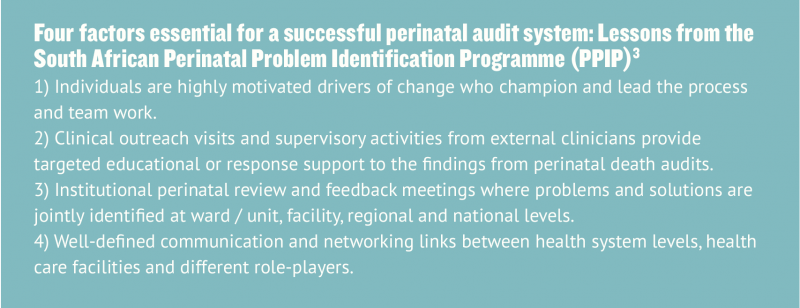
³ Belizán, M. Bergh, A-M. Cilliers, C. Pattinson, R.C. & Voce, A. for the synergy Group (2011) Stages of change: A qualitative study on the implementation of a perinatal audit programme in South Africa. BMC Health Services Research. 11:243
This post from a member of the Stillbirth Advocacy Working Group (SAWG) reflects the perspective of the author alone; it does not represent the views of the SAWG.
The Stillbirth Advocacy Working Group was founded by the Partnership for Maternal, Newborn and Child Health, and is co-chaired by the International Stillbirth Alliance and the London School of Hygiene & Tropical Medicine. Email co-chairs Hannah Blencowe or Susannah Leisher at hannah-jayne.blencowe@lshtm.ac.uk or shleisher@aol.com to learn more, or sign up to join the group here!